Nearly 4 million Americans live with fibromyalgia, and more than 1 million carry a diagnosis of multiple sclerosis — yet both conditions are routinely misdiagnosed as each other for years before patients receive the right answer. If you or someone you love has been told “we’re not sure what this is,” you are not alone, and you deserve clarity. As a trusted neurology doctor in Brooklyn, NY, AllHealth Diagnostic and Treatment Center sees this diagnostic challenge regularly, and this guide is designed to give your family the knowledge to move forward with confidence.
Trusted care Neurology doctor in Brooklyn, NY.
Key Takeaways
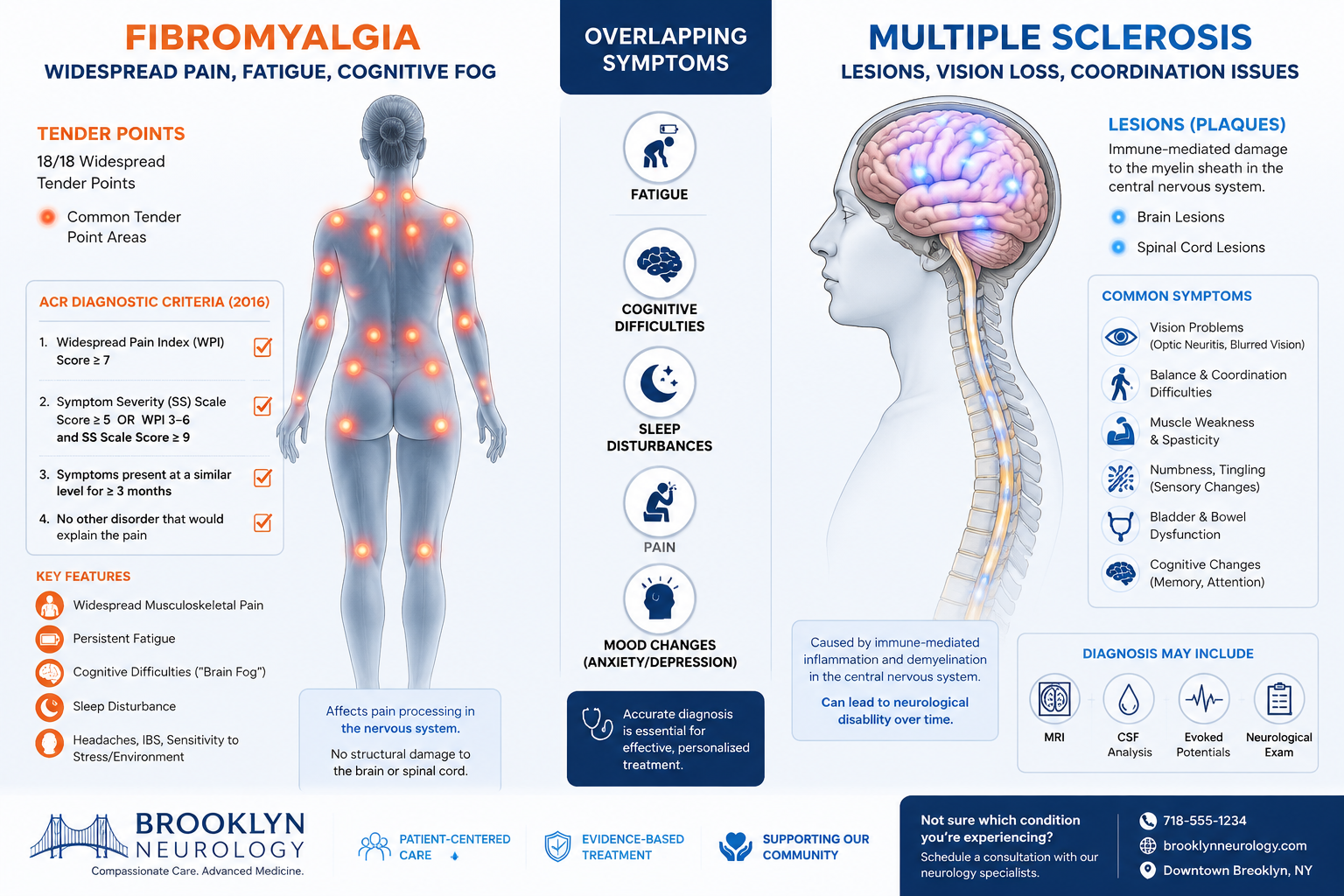
- Fibromyalgia and multiple sclerosis share overlapping symptoms — including chronic pain, fatigue, and cognitive difficulties — but they have fundamentally different causes and diagnostic pathways.
- MS is a structural, immune-mediated disease detectable on MRI; fibromyalgia involves no visible lesions or nerve damage on imaging.
- A formal fibromyalgia diagnosis follows the American College of Rheumatology’s 2016 criteria, while MS diagnosis relies on MRI, spinal tap, and evoked potential testing.
- Early, accurate diagnosis matters — the wrong treatment plan can delay meaningful relief for years.
- Seeing a qualified neurology doctor in Brooklyn, NY is the most important step you can take if symptoms are unclear or worsening.
Why These Two Conditions Are So Easily Confused
Both fibromyalgia and multiple sclerosis (MS) belong to a frustrating category of conditions: they are invisible to the naked eye, variable from day to day, and capable of mimicking dozens of other diseases. Patients often spend months — sometimes years — cycling through specialists before landing on the right diagnosis.
The confusion is understandable. Consider the symptom overlap:
| Symptom | Fibromyalgia | Multiple Sclerosis |
|---|---|---|
| Chronic widespread pain | Yes | Yes (neuropathic) |
| Fatigue | Yes | Yes |
| Cognitive difficulties (“brain fog”) | Yes | Yes |
| Sleep disturbances | Yes | Sometimes |
| Numbness or tingling | Sometimes | Yes |
| Vision problems | No | Yes |
| Coordination or balance issues | No | Yes |
| Slurred speech | No | Yes |
| Detectable MRI lesions | No | Yes |
| Bladder dysfunction | Rarely | Yes |
Comprehending what is the meaning of clinical diagnosis in medicine is essential here — because for both conditions, the clinical picture must be interpreted carefully and systematically, not rushed.
The Root Cause Difference
This is the most important distinction to understand:
- Fibromyalgia is a disorder of pain processing. The nervous system amplifies pain signals abnormally, but there is no physical damage to nerves, the brain, or the spinal cord. Think of it as a volume dial that is stuck too high.
- Multiple sclerosis is an autoimmune disease in which the immune system attacks the myelin sheath — the protective coating around nerve fibers. This causes real, measurable structural damage that shows up on imaging. Over time, MS can cause progressive neurological disability.
This distinction drives everything that follows: the tests ordered, the treatments prescribed, and the long-term prognosis.
Diagnostic Criteria: What a Neurology Doctor in Brooklyn, NY Looks For
Diagnosing Fibromyalgia: The ACR 2016 Criteria
Fibromyalgia has no blood test, no MRI finding, and no biopsy result that confirms it. Diagnosis is clinical — meaning it is based on a structured evaluation of symptoms. The American College of Rheumatology’s 2016 criteria require all three of the following:
- Widespread Pain Index (WPI) of 7 or higher and a Symptom Severity (SS) scale score of 5 or higher — OR a WPI of 4 to 6 combined with an SS score of 9 or higher.
- Generalized pain present in at least 4 of 5 body regions (left upper, right upper, left lower, right lower, axial).
- Symptoms present for at least 3 months at a similar level.
Importantly, a fibromyalgia diagnosis remains valid even when another condition is present. This means a patient can have both fibromyalgia and MS simultaneously — a scenario that makes accurate differential diagnosis even more critical.
Diagnosing Multiple Sclerosis: Objective Tests Required
Unlike fibromyalgia, MS diagnosis depends heavily on objective, measurable findings. A neurologist will typically order:
- MRI of the brain and spinal cord: This is the cornerstone of MS diagnosis. White matter lesions — areas of demyelination — appear as bright spots on specific MRI sequences. Their location, size, and pattern help confirm the diagnosis.
- Spinal tap (lumbar puncture): Cerebrospinal fluid is analyzed for oligoclonal bands and elevated immunoglobulin G (IgG) levels, which indicate immune activity in the central nervous system.
- Evoked potential tests: These measure how quickly the nervous system responds to stimuli (visual, auditory, or sensory). Slowed responses suggest demyelination along specific nerve pathways.
For patients who may also need EMG and nerve conduction studies, our neurology team at AllHealth DTC can coordinate this testing to rule out peripheral nerve disease — another condition that can mimic both fibromyalgia and MS.
MS-Specific Red Flags That Should Prompt Immediate Neurological Evaluation
If any of the following symptoms are present, a neurologist should be seen promptly — these are not consistent with fibromyalgia alone:
- Sudden or progressive vision loss in one eye
- Double vision
- Loss of coordination or balance (ataxia)
- Weakness in one or more limbs
- Slurred speech
- Bladder or bowel dysfunction with neurological features
- Symptoms that worsen with heat (Uhthoff’s phenomenon)
How a Neurology Doctor in Brooklyn, NY Approaches the Evaluation
When a patient presents with chronic pain, fatigue, and cognitive symptoms, a systematic approach is essential. At AllHealth Diagnostic and Treatment Center, our neurology team follows a structured evaluation pathway:
Step 1 — Detailed History The clinician asks about the onset, duration, pattern, and character of symptoms. MS symptoms often come in “attacks” (relapses) followed by partial or full recovery. Fibromyalgia symptoms tend to be constant but fluctuating, without clear relapse-remission cycles.
Step 2 — Neurological Examination A thorough physical exam checks reflexes, muscle strength, coordination, vision, and sensory function. Abnormal findings on exam — such as hyperreflexia, optic nerve changes, or gait abnormalities — point strongly toward MS rather than fibromyalgia.
Step 3 — Targeted Diagnostic Testing Based on the history and exam, the neurologist orders appropriate imaging and lab work. MRI is almost always ordered when MS is suspected. For fibromyalgia, labs are used primarily to rule out other conditions (thyroid disease, lupus, rheumatoid arthritis) rather than to confirm the diagnosis.
Step 4 — Integrated Interpretation Results are interpreted in the context of the full clinical picture. This is where experience matters most. Misreading a normal MRI as ruling out MS — or attributing all symptoms to fibromyalgia without proper workup — can lead to years of inadequate treatment.
Treatment Approaches: Why Getting the Diagnosis Right Matters
The treatment strategies for fibromyalgia and MS are fundamentally different. Prescribing the wrong approach not only fails to help — it can cause harm.
Fibromyalgia Management
- Medications: FDA-approved options include duloxetine, milnacipran, and pregabalin. Low-dose tricyclic antidepressants are also used for sleep and pain.
- Non-pharmacological approaches: Aerobic exercise, cognitive behavioral therapy (CBT), and sleep hygiene are among the most evidence-supported interventions.
- Lifestyle modifications: Stress reduction, pacing activities, and addressing sleep disorders are central to long-term management.
Multiple Sclerosis Management
- Disease-modifying therapies (DMTs): These are the cornerstone of MS treatment. They reduce the frequency and severity of relapses and slow disease progression. Examples include interferon beta preparations, glatiramer acetate, natalizumab, and newer oral agents.
- Relapse management: High-dose corticosteroids are used to shorten acute relapses.
- Symptom management: Physical therapy, occupational therapy, and medications for spasticity, fatigue, and bladder dysfunction.
For patients managing complex chronic conditions, our home care coordinator program can help ensure continuity of care between specialist visits — especially valuable for those with mobility challenges or multiple comorbidities.
Special Considerations for Families in Midwood and Flatbush
For families in our Brooklyn community, navigating these diagnoses can feel overwhelming — particularly when language barriers, insurance complexities, or cultural concerns add to the challenge. AllHealth Diagnostic and Treatment Center was built specifically to serve this community with warmth and without judgment.
A few points worth knowing:
- Children and adolescents can develop MS, though it is less common. If your child has unexplained neurological symptoms, our pediatric doctors can coordinate the appropriate referrals.
- Fibromyalgia is significantly more common in women, though it affects men and children as well. Hormonal factors may play a role, which is why our endocrinology services are often part of a comprehensive workup.
- Bladder symptoms — present in many MS patients — are also evaluated through our urology services in Brooklyn, NY, ensuring that no aspect of a patient’s experience goes unaddressed.
FAQs:
Can fibromyalgia and multiple sclerosis occur in the same person at the same time?
Yes. Both conditions can coexist. In fact, the American College of Rheumatology’s 2016 diagnostic criteria explicitly state that a fibromyalgia diagnosis is valid regardless of whether another condition is also present. This is one reason why a thorough neurological evaluation is so important — finding one diagnosis should not stop the search if symptoms remain unexplained.
Will a normal MRI rule out fibromyalgia or confirm it?
A normal MRI does not confirm fibromyalgia — it helps rule out MS and other structural conditions. Fibromyalgia produces no detectable changes on MRI because it is a disorder of pain processing, not a structural disease. A normal scan is consistent with fibromyalgia but must be combined with a full clinical evaluation using the ACR criteria to reach a diagnosis.
How long does it typically take to get a definitive diagnosis for either condition?
MS diagnosis can take anywhere from several weeks to over a year, depending on how clearly symptoms fit the diagnostic criteria and how quickly lesions appear on MRI. Fibromyalgia diagnosis has historically taken even longer — studies suggest an average of 2 to 5 years from symptom onset to diagnosis. Seeing a specialist early, rather than waiting, significantly shortens this timeline.
What should I bring to my first neurology appointment?
Bring a detailed symptom diary covering at least 4 to 6 weeks — note the type, location, severity, and timing of symptoms, as well as any triggers or patterns. Also bring a complete list of current medications and supplements, any prior imaging or lab results, and a list of questions. The more information your neurologist has at the first visit, the more targeted and efficient the evaluation will be.
References
- National Institute of Neurological Disorders and Stroke. (2023). Multiple sclerosis: Hope through research. U.S. Department of Health and Human Services. https://www.ninds.nih.gov/health-information/disorders/multiple-sclerosis
- National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2022). Fibromyalgia. National Institutes of Health. https://www.niams.nih.gov/health-topics/fibromyalgia
- Bhise, V., et al. (2021). Defining the clinical course of multiple sclerosis: The 2013 revisions — practical implications for clinical care. Multiple Sclerosis Journal, 27(5), 671–679. https://doi.org/10.1177/1352458521994045
- Centers for Disease Control and Prevention. (2022). Fibromyalgia. https://www.cdc.gov/arthritis/types/fibromyalgia.htm
Allhealth in Coney Island Avenue
1100 Coney Island Avenue,
2nd Floor, Brooklyn, NY 11230
Phone: (718) 942-4944
Email: IDD@allhealthdtc.com
Allhealth in East 13th Street
1655 East 13th Street,
Brooklyn, NY 11229
Phone: (718) 339-6900
Email: medical@allhealthdtc.com

